
Why Your Fascia Won't Change Until You Fix Your Tongue, Toes, and Eyes
Why your fascia stays dense and stuck despite stretching. Learn how sensory input from your feet creates compensation patterns fascia adapts to permanently.

In This Article, You Will Discover:
Why fascia does not create posture but adapts to the movement patterns your nervous system repeats.
How unresolved sensory mismatch in your foundation biases balance and motor output over time.
Why local fascial work can feel effective yet fail to hold once you return to normal movement.
What changes when the signal your brain relies on becomes clearer and more consistent.
Why correcting input precedes lasting change in tissue behavior and posture.
Test This Right Now
Stand barefoot. Close your eyes. Notice which foot feels more grounded. Now shift your weight slightly side to side.
Does one foot feel unstable? Does your body lean to compensate?
Open your eyes. That imbalance you just felt is something your nervous system has been managing for years, and your tissue has adapted to whatever pattern it repeats.
What Fascia Actually Does (And What It Doesn’t)
Fascia is connective tissue that wraps every muscle, organ, and structure in your body. It's supposed to be smooth, elastic, and organized in clean lines that follow the direction of force and movement.
But look at fascia under a microscope in someone with chronic pain or postural dysfunction, and you'll see something completely different: dense, irregular tissue that looks almost like scar tissue. Disorganized. Stuck. Resistant to change.
The fitness industry will tell you this is a hydration problem. Or a mobility problem. Or that you need specialized fascial training.
They’re wrong.
Your fascia looks like that because your brain has locked your body into a compensation pattern and your fascia is simply adapting to the posture your nervous system is forcing you to hold.
The Three-Point System Nobody's Connecting
Your fascia doesn’t organize itself. It responds to three primary sensory inputs your brain uses to map your body in space:
Your toes (foundation) - Pressure distribution from your feet tells your brain where the ground is and how to organize everything above it.
Your eyes (horizon reference) - Visual input controls head position, which dictates neck and upper body organization.
Your tongue (skull base anchor) - Tongue position directly influences jaw alignment, which affects the entire craniocervical system through the trigeminal nerve.
These three points form a neurological triangle. When any one is off, your brain compensates. Your fascia adapts to whatever compensation pattern your nervous system repeats.
What’s Breaking Down Your Posture?
Fascial Adaptation (The Body’s Response)

Fascia responds to mechanical demand. Whatever movement and tension patterns your body repeats, fascia reinforces over time.
If your nervous system consistently holds one shoulder forward to maintain balance, fascia will gradually adapt to support that position.
If your head shifts forward to stabilize vision, fascia along the neck and upper back will thicken to tolerate the repeated load.
This is not poor tissue quality. It is structural reinforcement.
Your fascia is doing exactly what it is designed to do. It adapts to the demands created by your nervous system.
The issue is not the tissue. The issue is that the demand is being driven by an inaccurate map.
The Compensation Loop That Never Stops
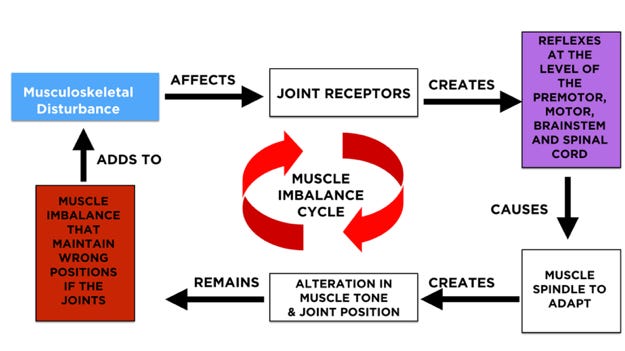
Here’s the cascade:
Step 1: Faulty sensory input from your feet, eyes, or jaw gives your brain an inaccurate map of where you are in space.
Step 2: Your brain settles into a compensation pattern to maintain balance and keep vision stable despite unclear input.
Step 3: That compensation becomes the pattern your body repeats, and your tissue adapts over time to support it.
Step 4: The adapted tissue limits movement options, which increases reliance on the same compensation pattern.
The Numbers No One’s Talking About
A 2011 study in BMC Musculoskeletal Disorders by Langevin and colleagues found that people with chronic low back pain showed 25% increase thickness in thoracolumbar fascia and 56% reduced shear strain (the ability of fascial layers to glide past each other) compared to healthy controls. But here’s what matters: the fascia didn’t create the problem. The postural compensation created the fascial changes.
The fascia didn’t need manual release. It needed the compensation pattern removed.
A 2016 follow-up study in PLOS ONE by Bishop and colleagues demonstrated that combining injury with movement restriction in an animal model produced a 52% reduction in fascial shear strain and these changes occurred in tissue away from the injured site. The body was reorganizing its fascia to support a new compensatory pattern throughout the entire system.
Multiple studies published in Experimental Brain Research (2005) and The Journal of Physiology (1999) showed that gaze direction alone where your eyes look directly modulates neck muscle activity, creating immediate changes in muscle tension patterns that persist as long as the visual input remains skewed. Your eyes control your neck. Your neck controls your fascia.
Your fascia isn’t broken. It’s responding accurately to a broken signal.
Why Fascial Training Takes So Long (And Why It Keeps Coming Back)

Fascial stretching, myofascial release, and hydration protocols all assume the fascia itself is the problem.
But fascia is the body’s most adaptive tissue. It responds to demand within hours.
Here’s what actually happens:
You can improve posture through fascial work, strength training, or movement patterns. People do it every day. But notice how long it takes weeks, months, sometimes years of consistent effort.
And notice what happens when you stop: the tension returns. The restriction comes back. Your body drifts back to the old pattern.
That’s not a failure of discipline. It’s your nervous system recreating the compensation pattern it never stopped receiving signals to maintain.
When you stretch tight fascia or train new movement patterns while your feet are still sending faulty pressure signals, you’re essentially overriding your brain’s automatic compensation through conscious effort and repetition.
It works. But it’s exhausting. And it’s temporary.
Because the neurological demand creating the fascial restriction is still active. Your brain is still receiving incorrect sensory input from your foundation. It’s still compensating to keep you upright despite faulty data.
You didn’t fix the signal. You just taught your body to work around it.
That’s why it takes months instead of weeks. That’s why constant maintenance is required. That’s why the same spots keep tightening back up.
You’re not treating the fascia. You’re fighting the signal.
Fix the signal first correct the sensory input from your feet, eyes, and jaw and your fascia reorganizes automatically. Not because you stretched harder or hydrated better, but because the neurological demand creating the dysfunction has been removed.
One approach works against your nervous system. The other works with it.
One takes months and requires constant reinforcement. The other takes weeks and becomes automatic.
Why Traditional Fascia Work Fails (And What Actually Works)
Most fascia protocols focus on releasing restrictions in your shoulders, neck, back, and hips—the middle of your body where you feel the tension.
But that’s not where the problem starts.
The tension in your upper traps isn’t creating your postural pattern. It’s adapting to it.
The restriction in your thoracolumbar fascia isn’t the driver. It’s the response.
Traditional approaches treat the middle while ignoring the endpoints—the top (tongue position, visual input) and bottom (foot pressure distribution)—that are creating the compensation pattern in the first place.
That’s why the same spots keep tightening back up. You’re releasing the adaptation without correcting the signal.
Here’s what changes when you fix the endpoints first:
You can improve posture by working on fascia, movement patterns, or strength for months.
Or you can correct the three sensory endpoints creating the compensation pattern in weeks.
The difference isn’t effort. It’s sequencing.
When you correct sensory input at the foundation—your feet, eyes, and tongue—your brain stops forcing compensations up the chain. The postural pattern changes. Your tissue adapts to the new demand.
Dense tissue becomes more elastic. Restricted movement becomes more available. Patterns become easier to change.
Not because you hydrated better or stretched harder, but because the neurological demand creating the dysfunction was removed.
The cascade:
Your brain no longer compensates to maintain balance on uneven foot pressure. The tension patterns your tissue has been reinforcing are no longer required.
Your head position stabilizes as visual input becomes consistent. Neck tension that kept returning reduces because the demand driving it is gone.
Jaw position normalizes, altering input to the skull base. Upper body restriction eases because the compensation pattern maintaining it is no longer necessary.
This isn’t about replacing fascial work or movement training. It’s about giving your nervous system accurate data first—so every other intervention works with it instead of against it.
Fascial training still works. Movement patterns still matter. When sensory input is corrected first, they work in weeks instead of months and require less constant reinforcement.
You’re not bypassing the tissue. You’re removing the neurological demand that keeps recreating the restriction.
The Foundation-First Reset Protocol
Most people start by treating their fascia directly—rolling, stretching, hydrating. That’s starting in the middle.
Here’s the correct sequence:
Step 1: Fix Your Foundation First
Your feet are the base of the entire sensory triangle. When foot pressure distribution is corrected, your brain stops compensating upward through your entire body.
The Therapeutic Insoles recalibrate the 200,000 mechanoreceptors in your feet, giving your brain accurate pressure data from the ground up. This is THE foundation that must be corrected before anything else will hold.
Start here. Everything builds from this.
Step 2: Retrain Visual Input
Your eyes are the second point of the sensory triangle. When visual input is skewed, your brain compensates by altering head position, which cascades through your entire fascial system.
The Brainpro App provides specific visual tracking exercises that recalibrate the horizon reference your brain uses to organize posture. These targeted eye workouts stabilize head position, which reduces the neurological demand creating neck and upper body fascial restrictions.
Fix your visual input, and the compensation patterns driven by unstable gaze begin to release.
Step 3: Lock In Tongue Position
Once your foundation is corrected, tongue and jaw position stabilizes the top of the triangle. The Functional Activator retrains proper tongue posture at the neurological level, correcting the skull base input that controls your entire upper body fascial organization.
Step 4: Let Your Fascia Reorganize Automatically
Once all three sensory inputs are corrected—feet, eyes, tongue—your nervous system no longer needs the compensation pattern. Your fascia adapts to the new demand within days to weeks. Not because you released it manually, but because the neurological signal changed.
Get the complete Sensory Reset Protocol →
What This Means for You Right Now
If you have been foam rolling the same areas for months with no lasting change, the fascia is not the primary problem.
If your neck tightens again no matter how much you stretch, the nervous system is recreating the pattern because the sensory input driving it has not changed.
If one side of your body consistently feels tighter, denser, or more restricted than the other, this is not asymmetrical tightness. It is asymmetrical compensation driven by uneven sensory input from your feet, eyes, or jaw.
This is not a tissue quality issue. It is a neurological organization issue expressed through tissue.
The Choice You’re Making Right Now
You can continue treating fascia as the problem through hydration, rolling, stretching, and release, and watch the same patterns return.
Or you can correct the sensory signals creating the compensation your tissue has been adapting to.
One approach manages symptoms. The other addresses the driver.
What you are seeing in the tissue is not a fascia problem. It is a nervous system problem expressed physically.
Correct the input. Tissue behavior follows.
What You’re Missing
The three-step protocol above gives you the framework. But there’s a critical fourth element I didn’t mention the one that determines whether your fascia reorganizes permanently or defaults back to compensation within weeks.
It’s called Sensory-Fascial Lock Release, and it’s the sequence that prevents your brain from recreating the old pattern.
This is the difference between temporary relief and permanent reorganization.
If you stop here, you’ll keep treating fascia as if it’s the problem. You’ll keep chasing hydration and mobility while your brain recreates the same stuck patterns.
Even after you correct foot pressure, visual input, and tongue position, your brain still remembers the old compensation pattern as "safe."
For the first 2-4 weeks after correcting sensory input, your fascia will reorganize. But without reinforcing the new pattern during this integration window, your nervous system will quietly revert to what feels familiar.
They corrected the input. But they didn't lock in the new pattern during the critical window.
Related reads to complete your posture correction:
References
Langevin, H.M., Fox, J.R., Koptiuch, C., Badger, G.J., Greenan-Naumann, A.C., Bouffard, N.A., Konofagou, E.E., Lee, W.N., Triano, J.J., & Henry, S.M. (2011). Reduced thoracolumbar fascia shear strain in human chronic low back pain. BMC Musculoskeletal Disorders, 12, 203. https://bmcmusculoskeletdisord.biomedcentral.com/articles/10.1186/1471-2474-12-203
Bishop, J.H., Fox, J.R., Maple, R., Loretan, C., Badger, G.J., Henry, S.M., Vizzard, M.A., & Langevin, H.M. (2016). Ultrasound evaluation of the combined effects of thoracolumbar fascia injury and movement restriction in a porcine model. PLOS ONE, 11(1), e0147393. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0147393
Bexander, C.S., Mellor, R., & Hodges, P.W. (2005). Effect of gaze direction on neck muscle activity during cervical rotation. Experimental Brain Research, 167, 422-432.
Grasso, R., Ivanenko, Y.P., & Lacquaniti, F. (1999). Effect of gaze on postural responses to neck proprioceptive and vestibular stimulation in humans. The Journal of Physiology, 519(1), 301-314.
Stecco, C., Stern, R., Porzionato, A., et al. (2011). Hyaluronan within fascia in the etiology of myofascial pain. Surgical and Radiologic Anatomy, 33(10), 891-896.
Schleip, R., Duerselen, L., Vleeming, A., et al. (2012). Strain hardening of fascia: Static stretching of dense fibrous connective tissues can induce a temporary stiffness increase accompanied by enhanced matrix hydration. Journal of Bodywork and Movement Therapies, 16(1), 94-100.
Mense, S. (2019). Innervation of the thoracolumbar fascia. European Journal of Translational Myology, 29(3), 8297.
Langevin, H. M., Bishop, J., Maple, R., et al. (2020). Effect of stretching on thoracolumbar fascia thickness and ultrasound echo intensity. Frontiers in Human Neuroscience, 14, 164.
Wilke, J., Macchi, V., De Caro, R., & Stecco, C. (2018). Fascia thickness, aging and flexibility: Is there an association? Journal of Anatomy, 234(1), 43-49.